Capitalism doesn’t just cut corners—it cuts people out. When “efficiency” becomes the only metric, anything that slows the system—complexity, ambiguity, difference—is branded as waste. In American healthcare that waste is measured not in dollars but in human suffering.
Fifteen‑minute visits. Specialists who treat only one body part at a time. Billing codes that reward neat closures over open‑ended inquiry. If your illness doesn’t fit a neat checkbox, you simply vanish from the data.
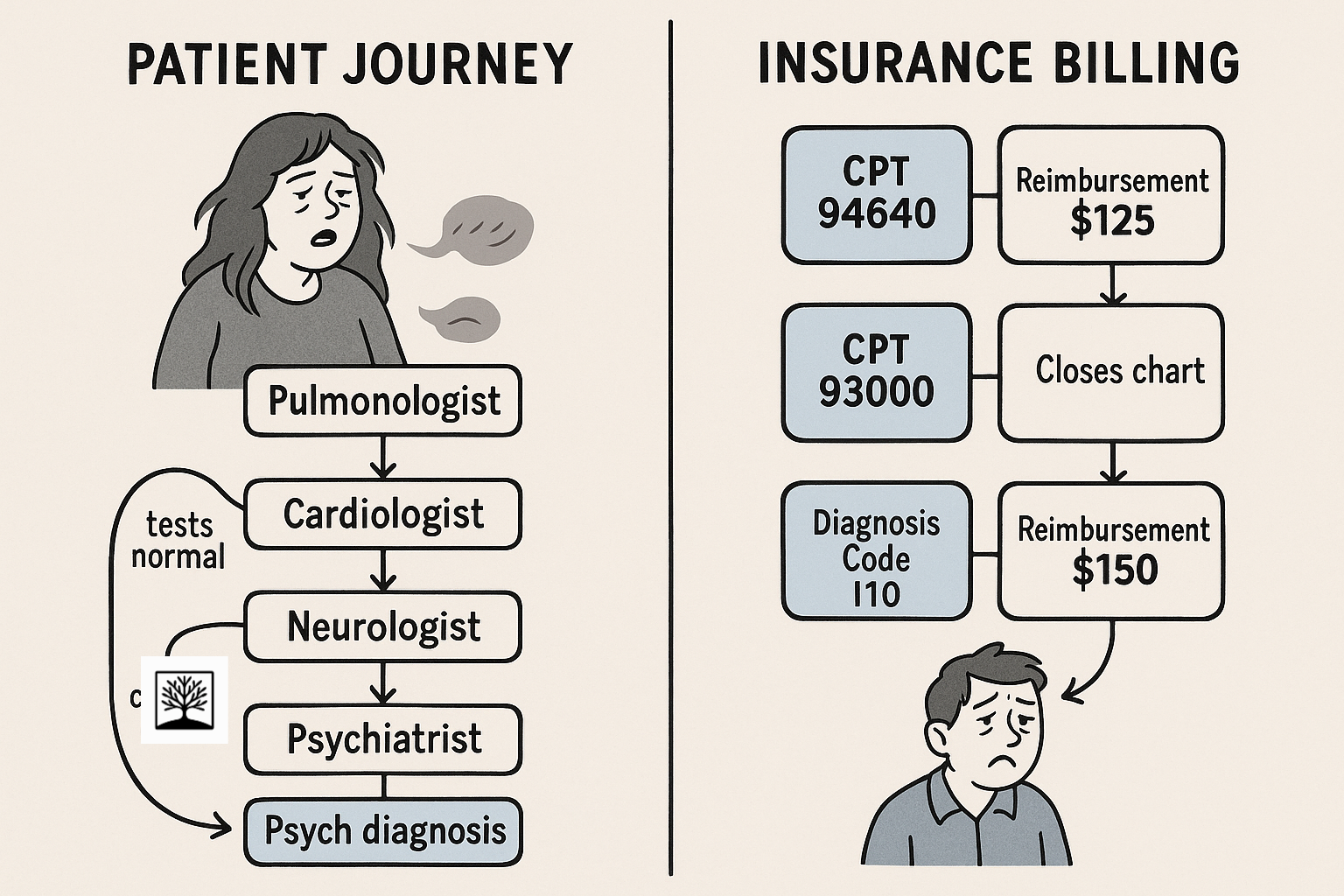
Take Long COVID: you wake breathless, heart racing, brain clouded, and are shuttled from pulmonologist to cardiologist to neurologist to psychiatrist. Every clinic runs its own tests, bills its own codes, and closes its chart. When each result lands “normal,” your record quietly morphs: your plea for help becomes “anxiety.” No one was paid to see the whole story, so the system recodes you as the problem.
This isn’t a rare glitch—it’s the blueprint. As I traced in Actuarial Medicine & Hidden Exclusion, our billing infrastructure sacrifices interpretive labor, pushing it—unpaid—onto those least able to carry it. What can’t be slotted into a clean code is either erased or pathologized.
Rare disorders fare no better. Ehlers–Danlos patients chase a genetic label for years, only to learn the multidisciplinary clinics they need are deemed “experimental” and excluded from coverage. ME/CFS sufferers, lacking a definitive biomarker, are sent into graded‑exercise regimens that deepen their collapse—and then denied disability. Without quantifiable proof, lived suffering becomes suspect.
Trans bodies face erasure by design. Electronic records force a “male” or “female” checkbox, so a trans man can’t book a Pap smear, and a trans woman can’t schedule a prostate exam. Gender‑affirming hormones are coded “cosmetic,” triggering Kafkaesque appeals. If your anatomy can’t be checked off, your care can’t be guaranteed.
Structural bias deepens the wound. Clinical algorithms—pain scales, kidney‑function formulas, fetal‑monitoring thresholds—rely on datasets calibrated on white men. When a Black mother’s labs stray, protocols don’t adapt; she disappears into statistical noise, helping explain why Black women die of pregnancy‑related complications three to four times more often than comparable white women.
“Universal” care, it turns out, defaults to whiteness.
These failures extend far beyond hospitals. In February 2021, Texas’s power grid—designed for summer profits—froze under Arctic winds. Engineers warned that pipelines needed insulation and turbines heaters, but winterization “didn’t pencil”; when pipes burst and hospitals went dark, dividends still cleared.
In 2023, Maui’s executives kept high‑voltage lines live through drought‑parched brush to avoid a one‑day revenue dip; Lahaina burned. Only lawsuits reframed “convenience” as criminal negligence, forcing mandatory shut‑offs.
Even aviation—the supposed gold standard of redundancy—succumbed when Boeing cut backup sensors from the 737 MAX to speed delivery. After two crashes and 346 deaths, they retrofitted safety features, solemnly branded “innovation.”
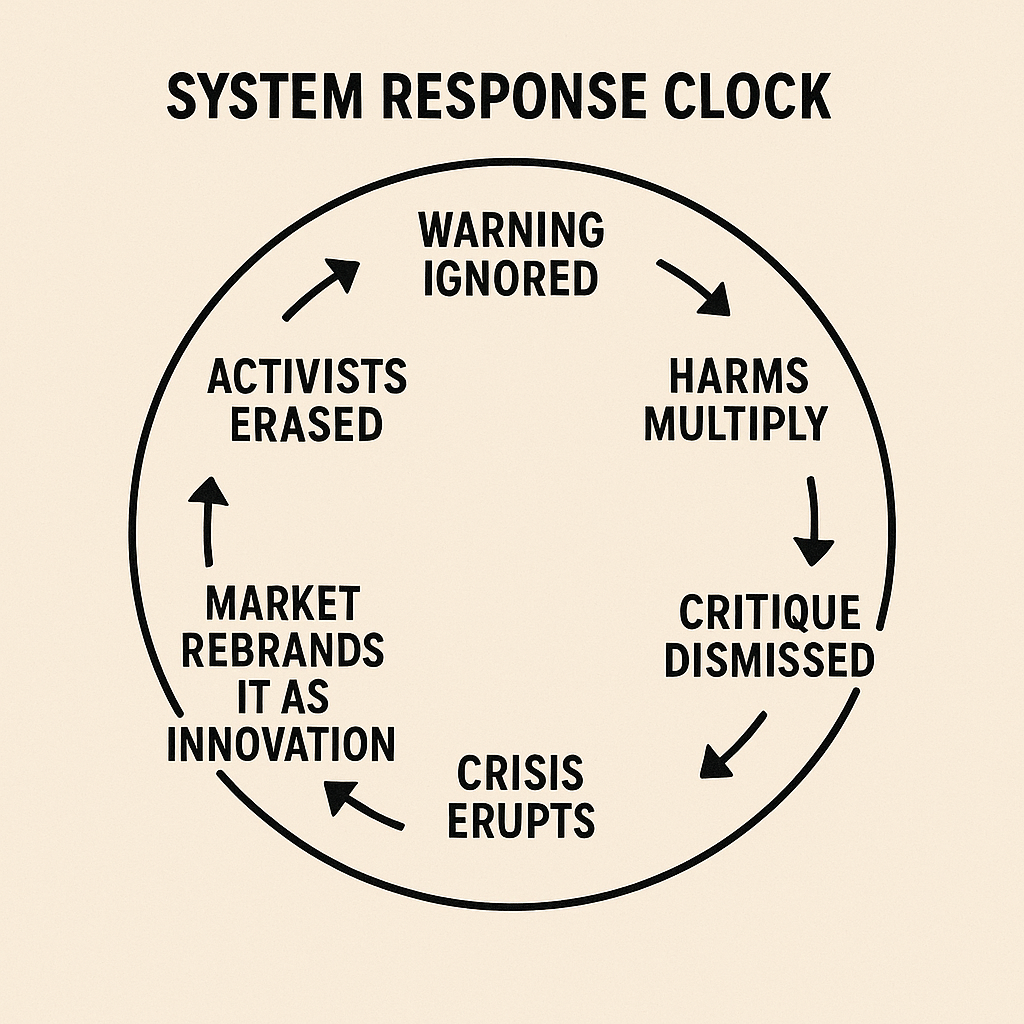
This cycle—neglect, collapse, retrofit, rebrand—is not a bug; it’s a feature. Institutions metabolize critique only once crises pay dividends to those who ignored early warnings.
Remote‑work tools championed by neurodivergent and caregiving professionals became “essential infrastructure” only after a pandemic threatened profits. Live‑captioning won by Deaf activism reappeared as a “new feature” when gyms and bars discovered they liked muted TVs.
That process of forgetting and rebranding is what I call The Amnesia Engine.
What if, instead of treating these edge solutions as extras, we baked them in from the start?
- Whole‑person clinics funded like trauma bays.
- Insulated pipelines and redundant sensors counted as essential.
- Slack in scheduling recognized as life‑saving capacity.
- Genuine trust in patient testimony honored as data.
These aren’t boutique R&D—they’re seat belts, fire codes, and stable grid design for society.
Yes, that costs more up front. But the true invoice for neglect arrives later—in lawsuits, funerals, and emergency interventions. Shuffling those receipts into another quarter and calling it “efficiency” is an accounting trick.
What looks like waste today often keeps tomorrow possible.
Edge‑case patients are not anomalies; they test the system’s limits in real life. Building a system that serves them well improves care for everyone.
When we refuse, we consciously let triage become our moral ceiling.
Thanks for reading syadvada! This post is public, so feel free to share it.